A couple of news reports I have read recently about this disorder disturbed me and in this post I try to dispel some widespread myths about it.
You must have read about Haemophilia in your 10th class Biology lessons. It is also known as The Royal Disease because it was first discovered in the royal family of England. Its incidence in the Russian Tsar (Czar)’s family has changed the course of world history during the World War I.
What is it at all? May be you were also dreaded that it is a very dangerous disease as there are several myths making rounds about it. Some of the widespread MYTHS are:
MYTH 1: It causes profuse bleeding. (Fact: bleeding is just normal)
MYTH 2: Even small cuts can be fatal. (Fact: Haemophilia affects the coagulation Factors which come into picture only when there is a major injury.)
MYTH 3: Haemophiliacs bleed to death. (Fact: here, at least three conditions are to be met:
1. The factor level is less than 1% which is an extremely rare case.
2. There should be a major injury where blood vessels are deeply cut.
3. No action is taken to stop the bleeding i.e., the injured may be unconscious and there is no one around to take care of him).
MYTH 4: There is no remedy. (Fact: There are no allopathic medicines yet but there are a number of remedies.
MYTH 5: It is caused by the deficiency of vitamin k. (Fact: Haemophilia is a genetic disorder)
There are some myths even among doctors. A friend of mine who is an MBBS doctor once opined that
(MYTH 6:) there can be haemophilic girls but no haemophilic women because they will bleed to death in their first menstruation! (Fact: See Myth 3 above.)
Fact: Depending on the factor levels, it takes longer for the bleeding to stop.
There are at least 15 factors and 5 proteins involved in the clotting process. All of them are numbered and some of them have common names as well, e.g.
Factor I: Fibrinogen,
Factor II: Pro-thrombin (this is usually inactive under the influence of anti-prothrombin called Heparin and becomes active when needed),
Factor III: Tissue Factor,
Factor IV: Calcium, etc. (Ca++ is essential in the coagulation process as a catalyst to spur factors like VII, IX, X XIII into action)
If Factor VIII is deficient, it is haemophilia Type A
If Factor IX is deficient, it is haemophilia Type B
In some cases, vWF may also be deficient or missing.
Factor levels:
• 25% to 150% of expected level is considered NORMAL.
• 5% to 25% is MILD haemophilia
• 1% to 5% is MODERATE
• less than 1% SEVERE.
Haemophilia is not a disease but a genetic disorder. It has two effects: 1. Prolonged bleeding and 2. swelling.
BLEEDING:
When the cut is minor, the blood vessel leading to the cut part contracts so that the amount of blood passing through it decreases and the wound heals without the need for any clotting process to take place.
When the cut is moderate, (a blood vessel is slightly cut), blood cells and fluid escape from the wound and the collagen fibres which are exposed initiate the clotting process.
Platelets rush to the spot to control the damage. Platelets release chemicals to attract more platelets. The accumulated and hardened platelets act like a plug to block the blood flow. This platelet plug is trapped in the mesh formed by the collagen fibres across the cut.
The clotting process starts with the thrombocytes releasing PF3.
PF3 + blood proteins -> Prothrombin
Prothrombin + Ca
++ -> Thrombin
Thrombin + Fibrinozen -> Fibrin (in Gel state) which forms a net trapping corpuscles to form the clot
When the cut is major, Clotting or coagulation factors cause fibrin to stick together and seal the wound.
The adhesion of platelets to the collagen is mediated by von Willebrand factor (vWF). vWF also binds to and stabilizes coagulation factor VIII. Binding of factor VIII by vWF is required for normal survival of factor VIII in the circulation.
SWELLING:
Swelling is internal bleeding. The bleeding may be in joints or in muscles. Bleeding in muscles is not a serious one which may last for a couple of days and usually heals itself. The patient has to be careful about bleeding (i.e., swelling) in joints because if unattended to, it may persist for longer periods and the joint may get damaged permanently and the pain is also unbearable in severe cases. The extent of swelling also depends on the factor levels and the severity of the sprain or hit.
WHAT CAN AND SHOULD HAEMOPHILIACS DO?
• They must do normal exercises regularly. This will strengthen the muscles and helps in fast recovery. Yoga and aerobics are highly recommended.
• They can play all outdoor games but must avoid risky, adventurous games (like boxing).
• When there is any swelling or bleeding, bed rest is advised.
• In emergency cases, to increase the factor level considerably, they can opt for blood transfusion, plasma transfusion, or Factor VIII injections.
• Bleeding in the head, haematuria (blood in urine), bleeding in the stomach are dangerous especially when factor level is less than 1%. style="font-weight: bold;">Rush to the hospital immediately.
• Before undergoing any surgery, they must tell the doctor that they are haemophiliac.
. They should not donate their blood (if the factor-deficient blood is given to another bleeding haemophiliac, bleeding does not stop as expected and in critical cases, the patient may die).
WHO WILL INHERIT HAEMOPHILIA?
Haemophilia is inherited only through X chromosome. But in females, if the second X chromosome is normal, they become only carriers. A carrier is just like a normal woman who never suffers from haemophilia (because of the presence of a normal X chromosome), but her children who inherit the wrong x chromosome from her will be affected.
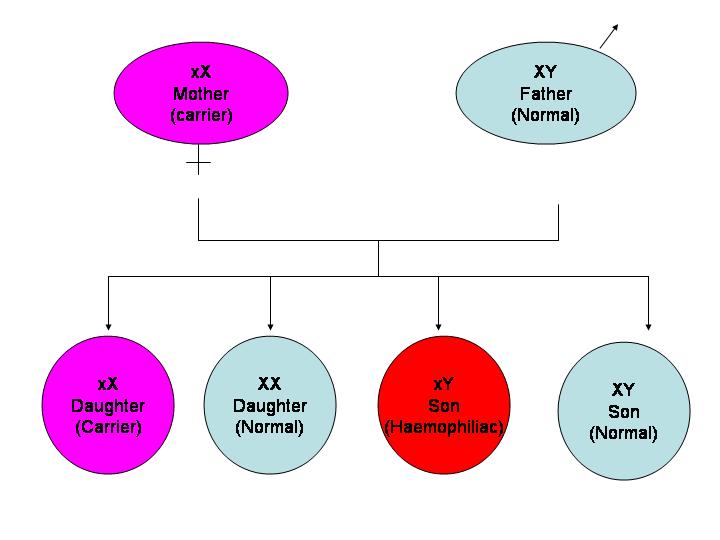
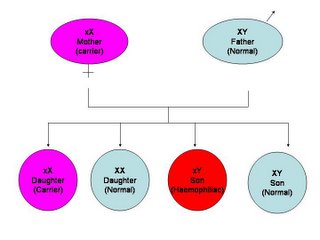
1. Children of a carrier mother and a normal father:
Daughters will be carriers with 50% probability
Sons will be haemophiliacs with 50% probability.
1. Children of a carrier mother and a normal father:
Daughters will be carriers with 50% probability
Sons will be haemophiliacs with 50% probability.
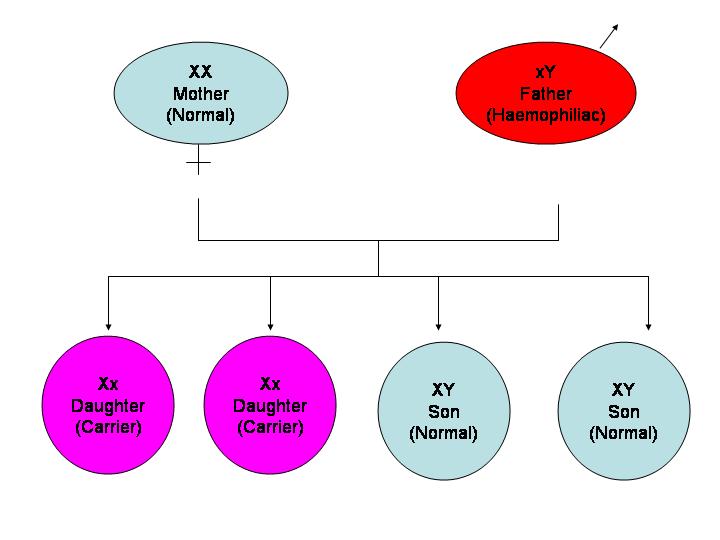
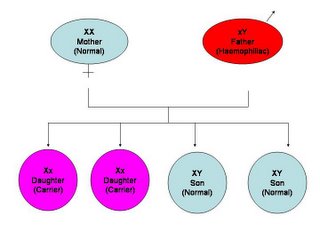
2. Children of a normal mother and a haemophiliac father:
All daughters will be carriers
All sons will be normal.
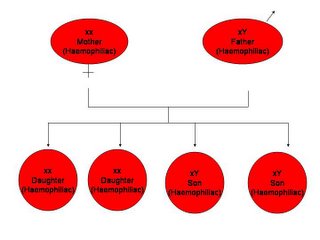
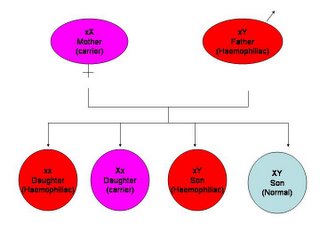
3. Children of a carrier mother and a haemophiliac father:
Daughters will be either carriers or haemophiliacs (No normal daughters)
Sons will be haemophiliacs with 50% probability.
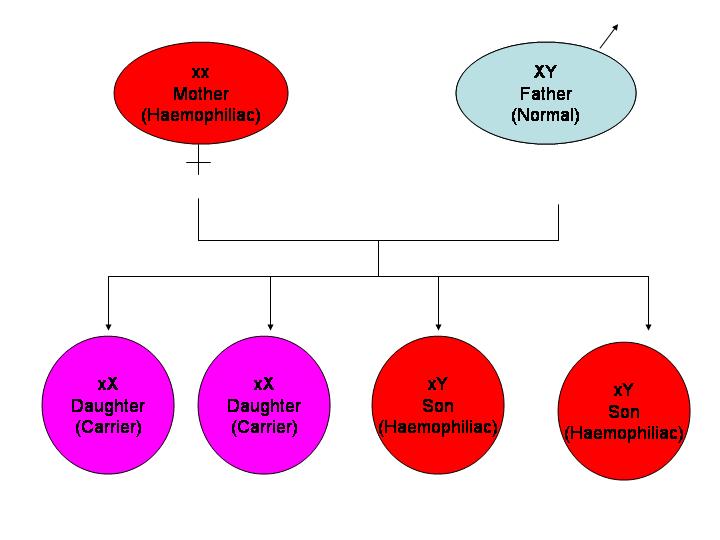
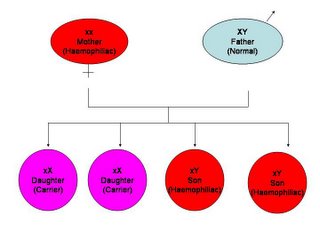
4. Children of a haemophiliac mother and a normal father:
All daughters will be carriers and all sons will be haemophiliacs.
5. Children of a haemophiliac mother and a haemophiliac father:
All children will be haemophiliacs.